AWA: Academic Writing at Auckland
Title: Public and political influence on Pharmac decisions
|
Copyright: Jack Reid
|
Description: Discuss why you think the general public and/or politicians should or should not have rights to influence Pharmac's decision to fund a drug? Use evidence from the scientific literature to make conclusions regarding whether you would support the financing of this drug by Pharmac.
Warning: This paper cannot be copied and used in your own assignment; this is plagiarism. Copied sections will be identified by Turnitin and penalties will apply. Please refer to the University's Academic Integrity resource and policies on Academic Integrity and Copyright.
|
Writing features
|
Public and political influence on Pharmac decisions
|
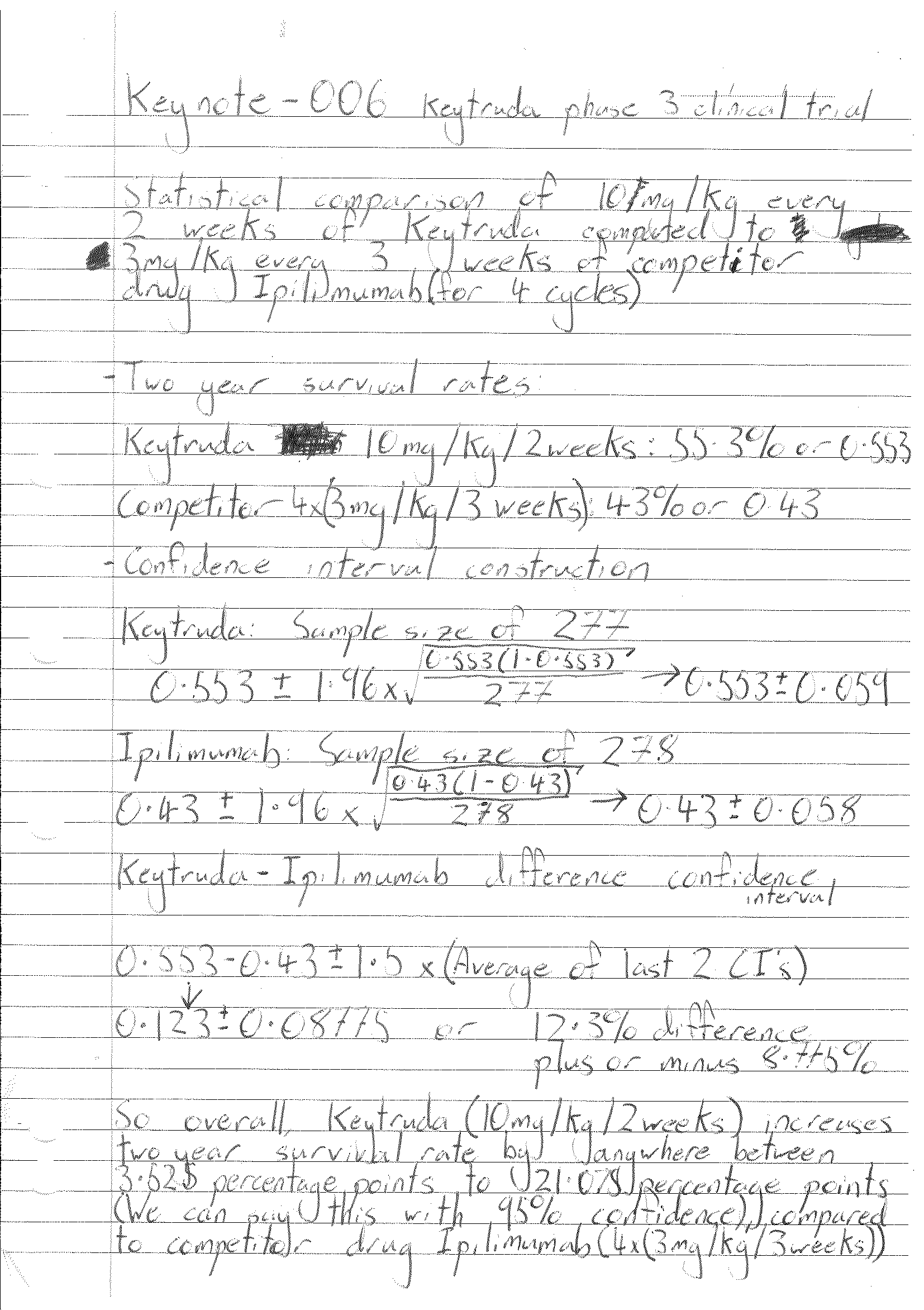
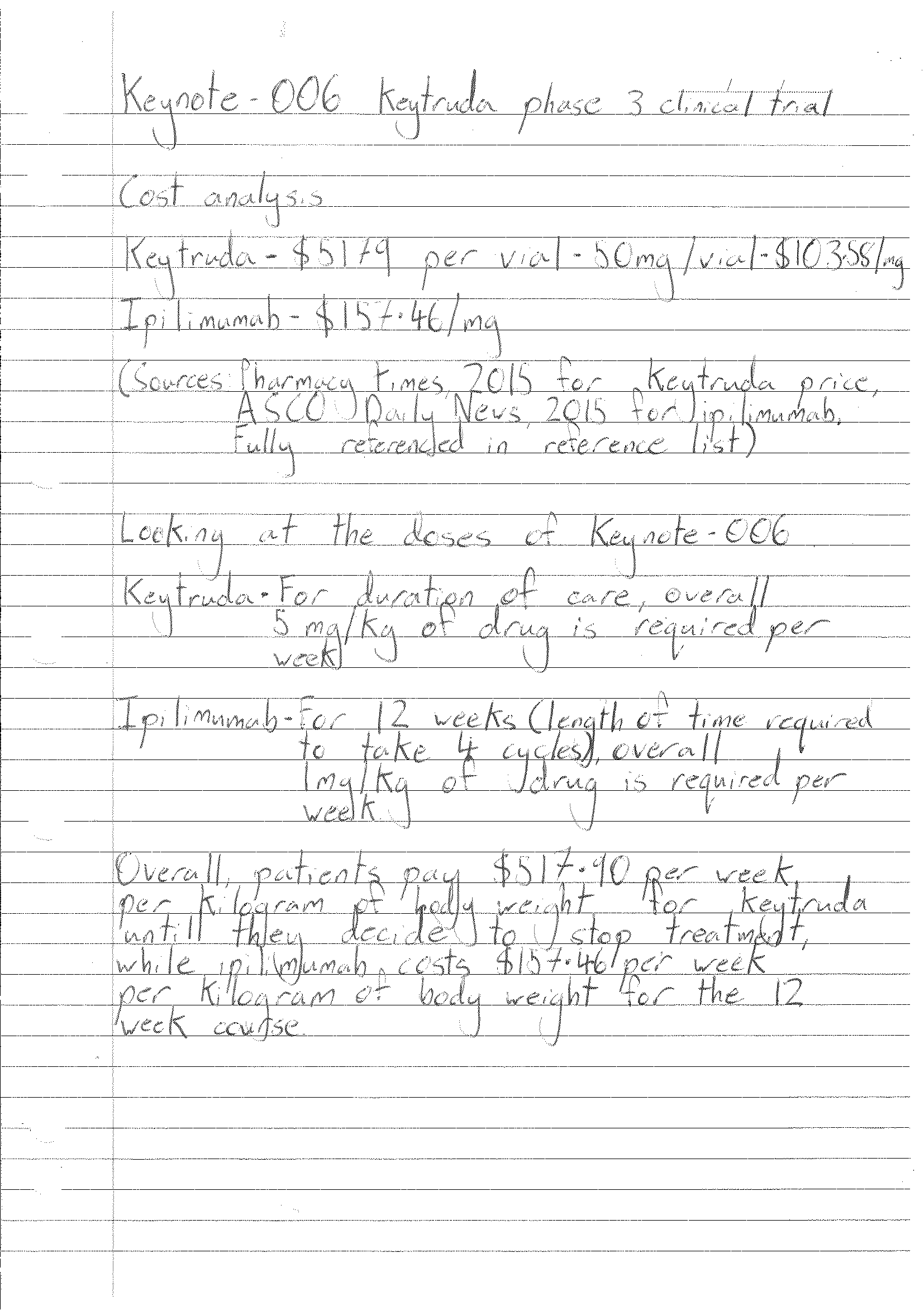
New Zealanders are paying too much for medicine. There’s a distinct lack of centralized negotiation which if implemented could drive pharmaceutical prices for all New Zealanders down. At least that is what the founders of what is now known as PHARMAC recognized in 1996-1999, when 4 independent government purchasing agencies came together with the vision of cheaper access to medicine for all New Zealanders (Gauld, 2014). PHARMAC has since both provided New Zealanders with cheap and affordable medication, but also has provided certain pharmaceutical companies with guaranteed sales and, with the help of government subsidies, a much wider market to sell their medicines to. PHARMAC has seen massive success in their goal, with drug prices plummeting (Duckett, 2013), governments around the world taking interest in PHARMAC’s cost cutting ability (Gauld, 2014), and even slowing the price increase of drugs compared to other countries (Cumming, Mays, & Daube, 2010). This success does not come without controversy. In recent months, the cancer drug Keytruda has been in New Zealand’s public spotlight because of controversial PHARMAC funding decisions. Keytruda is a drug used in patients with metastatic or unresectable melanoma stage III or IV which aids the patient’s immune system in fighting against cancer cells. It does this by blocking a pathway in which the cancer cells would use to avoid the immune system (Sharp & Corp, 2016b). There has been major controversy over the efficacy of the drug and whether PHARMAC should fund it or not. On one hand some members of the public want it funded, while experts at PHARMAC have recommended it be funded but with a low priority, and only in special circumstances. Should the general public or the government have a right to pressure and change PHARMAC decisions? Should Keytruda be given the funding that some members of the public believe it deserves? PHARMAC has operated relatively free from the politics of New Zealand since its creation (with only 3 instances of government interference to fund medicines it previously wasn’t going to) (MacDonald, 2011). This lack of interference has been what has made PHARMAC so successful in its goals to limit drug prices in New Zealand. According to Duckett (2013), the reason why PHARMAC is so effective is because “The Government has taken the politics out of price-setting”. In fact, Duckett then goes on to show that in Australia, medicines cost anywhere between 6 to 20 times more than in New Zealand. This leads to an overspending of around 3.5 million dollars per day (Duckett, 2013), which could be much better spent on additional medicines or generally in the health sector. For reference, pharmaceutical subsidy decisions in Australia are made by a committee within their department for Health and Aging, a committee open to the politics of the time. This in itself is clear evidence that PHARMAC decisions should not be open to the influence of the government if we don’t want prices as high as Australia. Another reason for keeping the government and the public out of PHARMAC decisions is the public’s lack of knowledge on the relevant subject matter, and their susceptibility to emotive arguments. Pharmaceutical funding decisions need to be made with clear logical reasoning, especially in PHARMAC’s case, as they have a set budget (Gauld, 2014). This means that if an expensive medicine comes onto the market, PHARMAC may need to cease or reduce funding to another important drug if they want to fund said expensive medicine. The general public simply do not have the training and experience necessary to decide on large scale funding which will affect the lives of thousands if not millions of people. A good example of the general public being swayed is the argument to fund Keytruda. Various claims about Keytruda’s efficacy have been made by members of the public which are unsupported by the scientific research behind the drug. In a stuff.co.nz article, a family spokesperson for a melanoma patient claimed that she believed that Keytruda would have saved her son’s life (Loren & Redmond, 2016), when the scientific literature showed “No clinical trial has yet shown that pembrolizumab increases the length of life for melanoma patients compared with other new melanoma treatments or standard chemotherapy” (PHARMAC, 2015). This shows us how emotion can easily cloud the judgement of the general public, and therefore why they should not be able to influence PHARMAC decisions. The public, due to their lack of knowledge and expertise on pharmacy, can believe over-exaggerated and sometimes false information. PHARMAC itself states, after a large public push for the funding of Keytruda, “there is a gap between the public’s perception of the benefits offered by pembrolizumab and the measured benefits seen in the clinical trials to date” (PHARMAC, 2015). Seeing as the public perception of a product can be misinterpreted through either misunderstanding or simply deception, this shows us that the public should not be allowed to influence PHARMAC decisions. When melanoma progresses to stage III or IV, it is dire for the patient. Both stages mean that the initial melanoma has spread from its original site to sites either around the original site (Stage III) or to completely new areas in the body, including major organs (Stage IV) (Cancer Research UK, 2016). In the specific types of melanoma that Keytruda is designed to combat (unresectable or metastatic (stage III or IV) melanoma), there is already no chance of removal by surgery, and only a small portion of medicines exist to combat the cancer. Keytruda is classed as an ‘immunotherapy’ drug (Sharp & Corp, 2016b), so it works to aid the immune system in fighting the cancer, rather than the drug fighting the cancer itself. Keytruda’s clinical trials thus far has proved some level of efficacy against this type of cancer. In its KEYNOTE-023 phase 1 clinical trial, Keytruda elicited some level of response in around three quarters of those who took the drug, with nearly one quarter of those being ‘very good partial responses’ (Kenilworth, 2015). These are promising results when looked at on their own, but the story changes when compared with other medicines. Keytruda may have some clinically proven efficacy, but to be considered for funding from PHARMAC, it must be considered against other similar medicines. In Keytruda’s Keynote 006 phase 3 clinical trial, it was compared with another immunotherapy called ipilimumab. Merck considered the two-year survival rate of those studied. It found that 55.3% of those taking 10mg/kg of Keytruda every 2 weeks survived for two years, while 43% of those taking 3mg/kg of ipilimumab every 3 weeks for 4 doses survived for 2 years. Upon statistical analysis of the clinical trial data (see figure 1), we can conclude that (with 95% confidence) Keytruda increases the two-year survival rate of patients by between as low as 3.525 percentage points and as high 21.075 percentage points. This data may seem conclusive as to which drug is better, but when price is factored in it does not look to be so. Ipilimumab costs $157.46/mg, and Keytruda costs $103.58/mg. When factored in to their dosage requirements, Keytruda costs $517.90 per week per kilogram of the patient’s body weight for the entire course of treatment, while ipilimumab costs only $157.46 per week per kilogram of the patient’s body weight for the 12-week course. To put that in perspective, if an 80kg patient were to go into treatment, when treated with ipilimumab the total cost would be 51,161.60 (assuming no change in weight throughout therapy). Keytruda on the other hand would cost . Evaluating the proposed difference in two-year survival rate compared to the total cost, it is clear that an increase in two-year survival rate of 3.525-21.075 percentage points is not worth the staggering difference in cost.97,184 (when used for the same length as the ipilimumab- this calculation does not take into account the fact the continued use of Keytruda is required to maintain results) In conclusion, PHARMAC’s decision making process is complex and requires much analysis into the medicines it chooses to fund. A main portion of the reason that PHARMAC is so effective in negotiating down drug prices is the lack of government interference in its decisions, as it decreases the ability of big pharmaceutical companies to influence funding decisions. The question of funding Keytruda may have set a worrying precedent of public over-reaching their bounds, and may cause other pharmaceutical companies to start trying to increase public support for their products. Therefore, the government and the general public should stay away from PHARMAC decisions. In the case of Keytruda funding, it should only be funded when other treatment options that are cheaper do not work or because there are too many or too strong adverse side effects for the patient to comfortably handle. Reference Cancer Research UK. (2016, July 18). Stages of melanoma. Retrieved October 3, 2016, from http://www.cancerresearchuk.org/about-cancer/type/melanoma/treatment/stages-of-melanoma Cumming, J., Mays, N., & Daube, J. (2010). How New Zealand has contained expenditure on drugs. BMJ, 340(may18 1), c2441–c2441. doi:10.1136/bmj.c2441 Duckett, S. (2013). Australia’s bad drug deal high pharmaceutical prices. Carlton, Vic.: Grattan Institute. Gauld, R. (2014). Ahead of its time? Reflecting on New Zealand’s Pharmac following its 20th anniversary. PharmacoEconomics, 32(10), 937–942. doi:10.1007/s40273-014-0178-2 Kenilworth, N. J. (2015, December 7). Responses observed in Three-Quarters of heavily Pre-Treated multiple Myeloma patients receiving KEYTRUDA® (pembrolizumab) combined with Lenalidomide and dexamethasone. Business Wire. Retrieved from http://www.businesswire.com/news/home/20151207005472/en/Responses-Observed-Three-Quarters-Heavily-Pre-Treated-Multiple-Myeloma Loren, A., & Redmond, A. (2016, August 28). Victory in Keytruda campaign comes too late for Jeff Paterson who passes away after cancer battle. Stuff.co.nz. Retrieved from http://www.stuff.co.nz/national/health/83630542/keytruda-campaigner-jeff-paterson-passes-away-after-cancer-battle MacDonald, N. (2011, June 13). Pharmac: The politics of playing god. Stuff.co.nz. Retrieved from http://www.stuff.co.nz/dominion-post/capital-life/features/5131037/Pharmac-The-politics-of-playing-god Pappas, A. L., Hanna, S., & PharmD. (2015, May 11). Keytruda by Merck. Retrieved October 3, 2016, from Pharmacy Times, http://www.pharmacytimes.com/publications/health-system-edition/2015/may2015/keytruda-by-merck Pharmac. (2015). Clinical review of pembrolizumab (Keytruda). Retrieved from https://www.pharmac.govt.nz/assets/pembrolizumab-summary-of-advice.pdf Pharmac. (2016, August 19). Proposal relating to pembrolizumab (Keytruda), nivolumab (Opdivo), posaconazole (Noxafil) and raltegravir (Isentress). Retrieved October 2, 2016, from https://www.pharmac.govt.nz/news/consultation-2016-06-28-pembrolizumab-nivolumab-posaconazole-raltegravir/ Sharp, M., & Corp, D. (2016a, May 18). New KEYTRUDA® (pembrolizumab) Data from KEYNOTE-006 and KEYNOTE-001 in Advanced Melanoma, Including Updated Survival Data, To Be Presented at 2016 ASCO Annual Meeting. Retrieved October 3, 2016, from Merck Newsroom, http://www.mercknewsroom.com/news-release/research-and-development-news/new-keytruda-pembrolizumab-data-keynote-006-and-keynote-0 Sharp, M., & Corp, D. (2016b). How does KEYTRUDA® (pembrolizumab) work in advanced Melanoma? Retrieved October 3, 2016, from https://www.keytruda.com/melanoma/how-keytruda-works/
Figure 1:
|
|